Return to Human Tumor Assay Journal Main Index Page
Immunotherapy: A prematurely-abandoned treatment option in ovarian and breast cancers
Clinical trials are warranted to test macrophage-activating biologic response modifiers administered following chemotherapy of ovarian and breast cancers. This is based on (1) striking in vitro findings in fresh human tumor cell culture assays, (2) supportive data from pilot clinical trials, and (3) a sound mechanistic rationale. I would advocate sequential administration of (1) assay-directed chemotherapy, (2) "non-specific" immunotherapy (e.g. antigens derived from bacteria), and (3) more "specific" cytokine therapy (e.g. interferon gamma).
In 1991, my colleagues and I published a study1,2 in the Journal of the National Cancer Institute which I hoped would receive scrutiny and follow-up. This was a tumor immunology study which grew out of a contract research project. Continuing this research was at the time not an option, as my priorities were to establish a clinical laboratory to provide cell culture drug resistance testing.
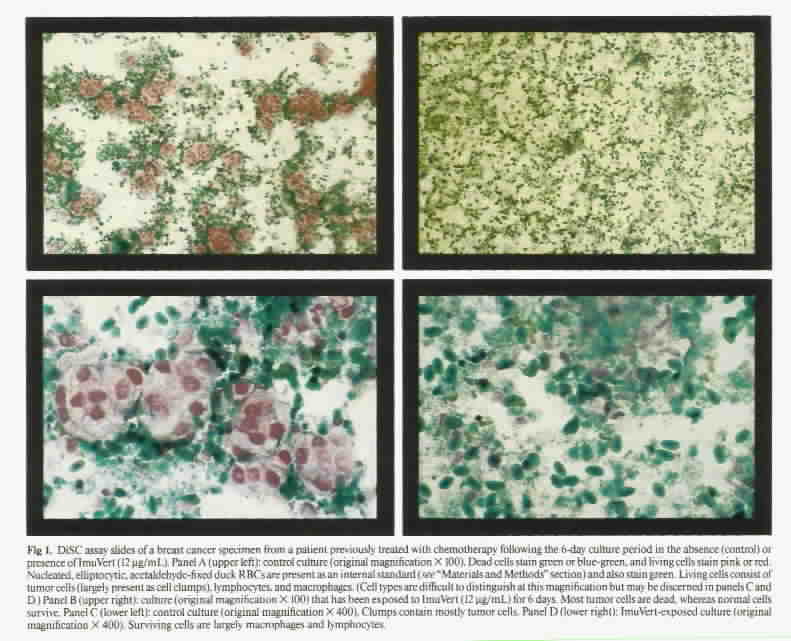
In the 1991 study, we presented the concept of "in situ vaccination," based upon our studies of biologic response modifiers in the DISC assay. We found that there was a striking association between the activity of biologic response modifiers which activate macrophages and the prior treatment status of patients with breast and ovarian cancers. Click here for color photomicrographs illustrating method .
The following agents were dramatically more active in fresh tumor specimens from previously-treated breast and ovarian cancer patients than against specimens from untreated patients:
1. ImuVert (a potent macrophage activator derived from Serratia marcescens)
2. Interferon gamma, and
3. Tumor necrosis factor
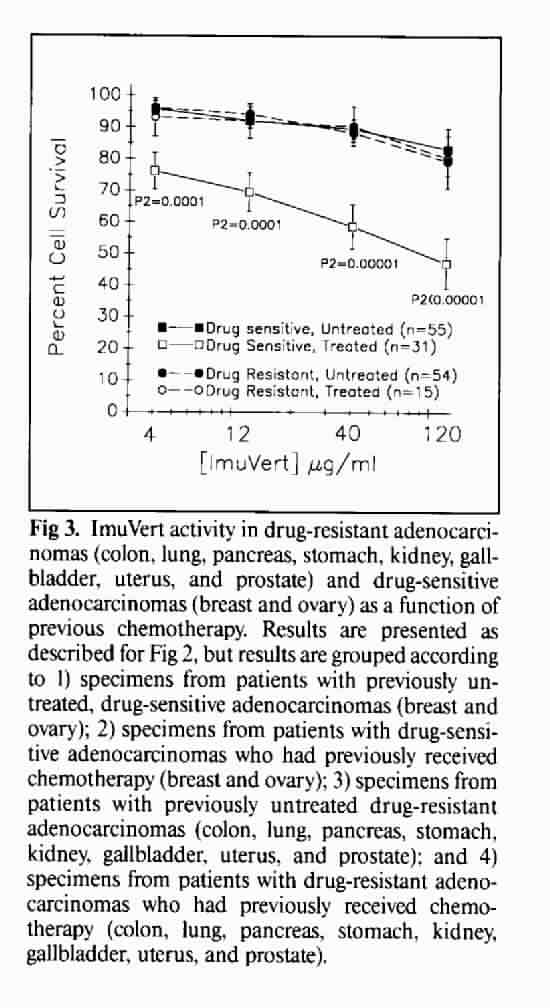
This greater activity in specimens from treated versus non-treated patients was not observed in adenocarcinomas known to be relatively resistant to chemotherapy (colon cancer, non-small cell lung cancer, etc.). Click here for graphs showing representative results.
This differential activity was also not observed in agents which are not potent macrophage activators (interleukin-2 and interferon alpha).
Based on these findings (and supported by anecdotal studies in the clinical trials literature), we proposed that effective chemotherapy produces massive release and processing of tumor antigens, which leads to a state in which the human immune system is primed (via "in situ vaccination") to respond to exogenous macrophage-activation signals with potent, specific antitumor effects.
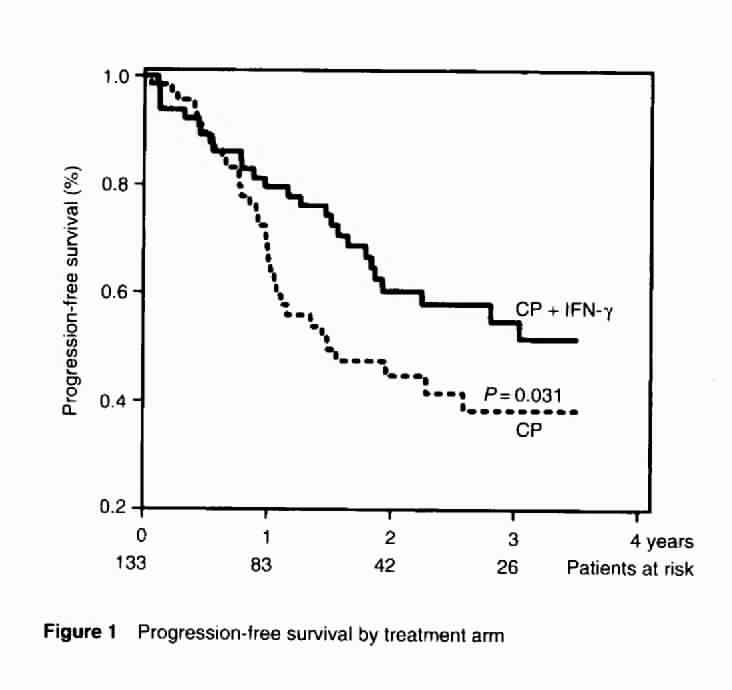
In the above-quoted study1, I reviewed a diverse clinical trials literature which supported this concept. More recently published was a randomized trial in previously untreated ovarian cancer3 , in which cisplatin/cyclophosphamide was compared to the same chemotherapy plus interferon gamma, administered subcutaneously three times a week, every other week, for the duration of chemotherapy (6 plannned treatment cycles). The study was prematurely closed because chemotherapy standard treatment had changed from platinum/cyclophosphamide to platinum/Taxol, but, even with the low power of the small numbers of patients accrued to show a difference, there was a significant advantage to combined treatment in progression-free survival (click here for progression-free survival curves) and a soft trend for improved overall survival. The authors quoted our earlier work1 in providing a mechanism for their positive results and called for follow-up clinical trials.
As noted above, my preferred trial design would be (1) first complete (preferably assay-directed) chemotherapy, then (2) administer non-specific immunotherapy to responders, then (3) provide more specific cytokine therapy, e.g. interferon gamma.
Literature Cited
1. Weisenthal LM, Dill PL, Pearson FC (1991) Effect of prior cancer chemotherapy on human tumor-specific cytotoxicity in vitro in response to immunopotentiating biologic response modifiers. J Natl Cancer Inst 83: 37-42
2. Weisenthal LM (1991) Effect of prior chemotherapy on biologic response modifier activity. J Natl Cancer Inst 83: 790-791
3. Windbichler GH, Hausmaninger H, Stummvoll W, Graf AH, et al. (2000) Interferon-gamma in the first-line therapy of ovarian cancer: a randomized phase 3 trial. Br J Cancer 82:1138-1144, 2000.
{kind=link}
{kind=link}
{kind=link}
{kind=link}