My response to ONCOLOGY's single written review provided to me:
November 30, 2001
James F. McCarthy Senior Vice President, Editorial
ONCOLOGY
48 South Service Road
Melville, NY 11747
Dear Mr. McCarthy:
I am in receipt of your letter of November 29, 2001, informing me that
you are unwilling to give me the opportunity to respond to the critique
of the reviewer and submit a revised manuscript. While your letter of December
6, 2000, along with my agreement to prepare the manuscript, may not have
constituted a contract, I do feel that we at least had a good faith covenant,
and I am going to ask you and your editorial board to deal with me in good
faith.
There are several relevant issues to consider:
1. In your letter of December 6, 2000, you pointed out that each paper
is referred to one or two reviewers, who are asked to write a short commentary
to be published alongside the paper. You stated the following: "The
commentary might be entirely laudatory, highly critical, or somewhere in
between. In any case it will serve to highlight areas of consensus or disagreement
among people most familiar with the topic in question. The result should
be both lively and informative."
Now, certainly you knew in advance of your invitation that this was a highly
controversial topic. Furthermore, you certainly knew that the preponderance
of clinical opinion was against the clinical use of these assays. I could
have written (and still can revise the manuscript to present) a more dispassionate
and less controversial discussion. I think that perhaps my (highly defendable)
criticism of current drug selection methods as being unblinded as to profit
margin may have struck a particularly sensitive nerve. But this point is
not central to the overall scope of the paper, and it could be omitted,
along with certain other controversial statements. But my point is this:
given the wording of your invitation, I had every reason to believe that
you wanted me to take a stand that was both honest (from my point of view)
and blunt. You invited controversy, and I gave you what you asked for.
2. Let's now look at the manuscript review provided to me. You state that
"the science just doesn't support the clinical recommendations,"
and that this is the basis of your rejection. I note once again that no
one has found fault with the scope, completeness, or accuracy of my review.
I worked very hard on ensuring that I was writing the most comprehensive
and accurate review ever written on the subject (I have previously contributed
a number of prior reviews to the literature, though none in the past 5
years, during which time there have been some very important new studies
published). So you asked me to review the topic, and I still have no reason
to believe that I in any way failed to do a good job in my review.
So the point of your dissatisfaction would appear to be centered around
what I conclude from these data, versus what your editorial board concludes.
You reject the paper because the science doesn't support the clinical recommendations.
But I make no specific clinical recommendations. I just conclude that the
tests "should be much more widely utilized in clinical oncology practice
and as an integral component to ongoing and future clinical trials."
Now, I think that the above point of view is highly defensible, but it
may certainly be criticized. That is what you had in mind, I believe, when
you asked me to write the paper. I review the literature. I arrive at certain
conclusions. Then the reviewers write rejoinders and you publish both.
If the literature do not support the current use of these assays, then
this is a point which deserves to be made, because these assays ARE being
rather widely used in everyday clinical oncology practice, in this country.
Most of the major laboratories are located here in California, although
specimens are submitted from all parts of the USA, including from many
NCI-designated comprehensive cancer centers. All the California managed
care organizations have approved payment for this testing and routinely
do pay. The California Medicare contractor has officially approved payment,
and this means that any Medicare patient anywhere in the USA can have his/her
tumor sent for testing, and Medicare will and does pay for the testing.
The technology has twice undergone rigorous evaluation by the nationally-respected
California Blue Shield technology assessment committee and both times was
unanimously approved for routine payment, which is routinely provided.
Approximately 10% of all ovarian cancer patients receive assay-directed
chemotherapy in the USA; I think that the number of assays currently being
performed on a non-investigational basis is on the order of 1,500 per month
in the USA. These are a lot of patients, and this is a lot of assay-directed
chemotherapy and a lot of money. If all of this is inappropriate and even
dangerous, then this should be brought to light and should not be buried.
My manuscript (which, again, is up to date and comprehensive...save for
a couple additional papers published since I wrote it, which I could include
in a revision) makes the best case for clinical use of the assays. If this
case falls short, then why not have two excellent clinical oncologists
expose the shortcomings of the data which support 1,500 assays per month
and Medicare reimbursement and Blue Shield reimbursement and managed care
reimbursement?
3. I would like to briefly address the issues raised by the written review
you provided to me (I will spare you the point by point rebuttal, which
I could certainly provide, but will not, as I want to be constructive and
not contentious). The reviewer takes a very narrow point of view, looking
only at ovarian cancer. In addressing the general point of view that these
assays "should be much more widely utilized in clinical oncology,"
by focusing solely on ovarian cancer, I believe the reviewer certainly
leaves out many clinical situations where the use of the assays is highly
defensible, in the context of the data presented in my review.
But let's just consider ovarian cancer; as noted 10% of all ovarian cancer
patients in the USA are currently being managed with regard to data provided
by cell culture drug resistance testing.
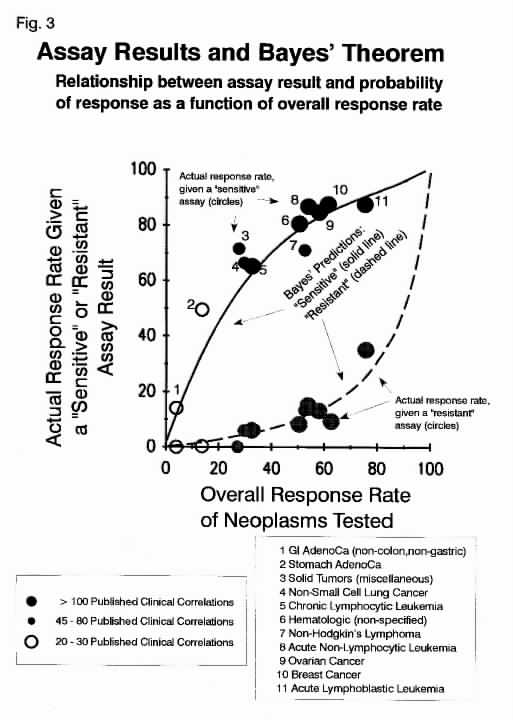
1. In the reviewer's correlation of assay findings with response, he/she
doesn't understand or consider the Bayesian statistics which apply to this
and all other diagnostic and predictive tests, including radiographic tests.
"True positive" and "true negative" rates for any test
(including the use of barometric pressure as a predictor of rain), vary
according to the "expected" or "pre-test" probability
of something happening. This is precisely the point illustrated in the
data shown in Figure 3 in the manuscript.
The cell culture drugs resistance tests are VERY accurate. Just as a barometric
pressure reading with a precision $1,000 German barometer is very accurate.
When the barometer says that the atmospheric pressure is rising, you can
believe what it says. But how does this help us in predicting weather?
It helps in the following way: absent a barometric pressure reading, all
we have is historical experience. In Southern California in November, there
is about a 10% chance of rain on any given day. With a rising barometer,
this decreases to less than 4%. With a falling barometer, the chance of
rain increases perhaps to 35%. So the instrument is: (1) "accurate"
(in correctly measuring atmospheric pressure) and (2) useful (in more clearly
defining the probability of rain). Note that the instrument is "accurate,"
but the correlation is only "useful," but not perfect. To take
this analogy one step further, let's move the barometer to Boston (still
in the month of November). In Boston, historical experience indicates that
there is a 30% chance of rain on any given day. With a rising barometer,
this falls to less than 10%. With a falling barometer, this increases to
more than 70%. Note that the accuracy of the instrument in measuring barometric
pressure hasn't changed, but the correlation has changed (the instrument
is still "useful," as it's much better to decide to play golf
on a day with a 10% chance of rain than with a 70% chance of rain, even
though the correlation between barometric pressure and actual weather is
not perfect.
The assays are very similar to the above analogy. They are VERY accurate
in measuring tumor cell death in the laboratory. Tumor cell death in the
laboratory clearly correlates with tumor cell death in the patient. Drugs
are more likely to kill tumors in patients in cases where they have been
found to kill tumors in the laboratory (and not to kill tumors in patients
in cases where they don't kill tumors in the laboratory). But the precise
correlations vary according to the underlying probability of the drugs
working on average, based on historical experience, just as in the case
of historical experience with probabilities of rain on any given day in
either Southern California or Boston in November. Just as with barometric
pressure, the correlation is about 7:1, meaning a seven-fold greater probability
of clinical benefit for drugs with good activity in the laboratory, compared
to drugs with poor activity in the laboratory (or a seven-fold greater
probability of good weather with a rising barometer than with a falling
barometer).
Let's take a few examples:
Previously-untreated breast cancer. Historical probability of clinical
benefit with Adriamycin = 50%. Theoretical probability of benefit with
a favorable assay = 80%. Theoretical probability of benefit with an unfavorable
assay = 11%
Previously-untreated colon cancer Historical probability of clinical benefit
with 5FU = 20%. Theoretical probability of benefit with a favorable assay
= 38%. Theoretical probability of benefit with an unfavorable assay = 4%
Previously-treated colon cancer Historical probability of clinical benefit
with irinotecan = 15% Theoretical probability of benefit with a favorable
assay = 29% Theoretical probability of benefit with an unfavorable assay
= 3%
And so on. The relationship between the historical "expected"
probability of response to chemotherapy and the more clearly-defined "assay-predicted"
probability of response is shown in the enclosed
graph.
Now, the value of the above information varies with different clinical
situations. In some situations, it might be of only negligible value and
might not be cost effective. But in other situations, it may be of considerable
value. But this holds for every laboratory and radiographic test in medicine.
Some clinicians use tests wisely; others use them unwisely. But the fact
that tests may be misused does not negate the value of tests in situations
where their utilization is helpful.
2. Clinical trials. The most valid criticism of the tests, in my opinion,
is that no one has ever completed prospective, randomized studies to show
that using the tests makes a difference in treatment outcome (n.b. two
controlled, non-randomized trials have been published, each showing highly
positive results, as described in the review). This is a completely valid
criticism. But it has to be pointed out that no laboratory or radiographic
tests in clinical oncology have ever been shown to make a difference in
treatment outcome. Perhaps these tests are somehow different than the use
of panels of expensive immunohistochemical stains to help diagnose and
classify tumors when such testing is performed for the purpose of selecting
chemotherapy. If so, these arguments could again be made in the accompanying
published critiques.
3. Response as a measure of benefit. The reviewer seems to agree that selection
of active first line therapy is important with respect to survival, but
questions the relevance of 2nd line therapy to survival. But this is not
a criticism of the assays; it is a more general criticism of 2nd line therapy.
Response is certainly considered important in 2nd line therapy. When response
occurs, therapy is continued. When response doesn't occur, therapy is discontinued
or changed. Therefore the relevance of identifying the most active drug(s)
would appear not to be controversial, at all. What is a matter for debate
(which is precisely what the manuscript was designed to promote) is whether
or not the assays should be used to assist in drug selection.
In point of fact, there are many different forms of 2nd line treatment:
platinums, topotecan, Doxil, etoposide, gemcitabine, gemcitabine combinations,
tamoxifen, hexamethylmelamine, and many other potentially reasonable treatments
(vinorelbine, docetaxel, 2nd line platinum combinations, etc.). A legitimate
point for consideration is whether or not the whole of the published literature
(considering all forms of cancer which comprise the entire published dataset),
supports the current use of these assays in assisting with this selection.
4. Cost benefit analysis. As you well know, very little in clinical oncology
has been subjected to rigorous cost-benefit analysis. None-the-less, the
points raised by the reviewer constitute a counter-argument to the positions
taken by me in my discussions of the meaning of the data presented in my
review. It would be highly appropriate to publish this counter-argument;
the importance of doing this is precisely because these tests are being
so widely used (and reimbursed), and their use is growing in this country.
If the current data do not support this, then is it not important to bring
this to the attention of the readership of ONCOLOGY? (of course, I could
provide counter-counter arguments to support my point of view; though your
reviewers would have the last word on this).
Reviewer's concluding remarks:
The reviewer's discussion of first line treatment of ovarian cancer actually
makes a defendable case for the use of the assays in this situation. The
reviewer correctly points out (as did I, in my own discussion presented
in the review) that "vast numbers of studies even in front line have
failed to consistently prove superiority of a combination over platinums
by themselves." And yet what is "standard" first line therapy
of ovarian cancer in the USA? Carboplatin + paclitaxel. This is much more
expensive than carboplatin alone. What about using the assays to determine
if carboplatin should be given alone, or with paclitaxel, or perhaps with
another drug (e.g. gemcitabine)? The arguments and counter-arguments which
are relevant to this question would make for an interesting debate.
Of great practical relevance is that these arguments have been made and
continue to be made on a regular basis in this country in the context of
reimbursement decisions. This again speaks to the relevance and importance
of a scholarly consideration of these issues in your journal.
With regard to the anecdote of gemcitabine/cisplatin, the reviewer states
that the advancement of this combination would have occurred absent the
use of the assays. This is no doubt true, but the point was that the clinical
use of the assays did clearly advance the clinical trials of this combination,
and the several clinical anecdotes provided (including the ovarian cancer
patient who failed first line carboplatin/Taxol (primary resistance), then
failed tandem high dose therapy with stem cell transplants (primary resistance),
only to subsequently achieve a durable CR with assay-directed gemcitabine/platinum,
does provide support for (though certainly, by itself, does not make the
entire case for) a role for currently-available cell culture drug resistance
testing in at least certain clinical situations.
Once again, you invited me to prepare a complete and accurate review of
the published data, for the point of stimulating debate on whether or not
these data are sufficient to support the current, rather widespread and
growing, use of these assays. I believe that I did exactly what you asked
me to do, and I cannot understand why you are not making a good faith effort
to work with me on revising this review to meet your worthy objectives.
Sincerely yours,
Larry M. Weisenthal
{kind=link}