Chapter 3: Correlations between cell death assay results and chemotherapy response
The hypothesis to be tested with clinical correlations was a very simple one - that above-average drug effects in the assays would correlate with above-average drug effects in the patient, as measured by both response rates and patient survival.
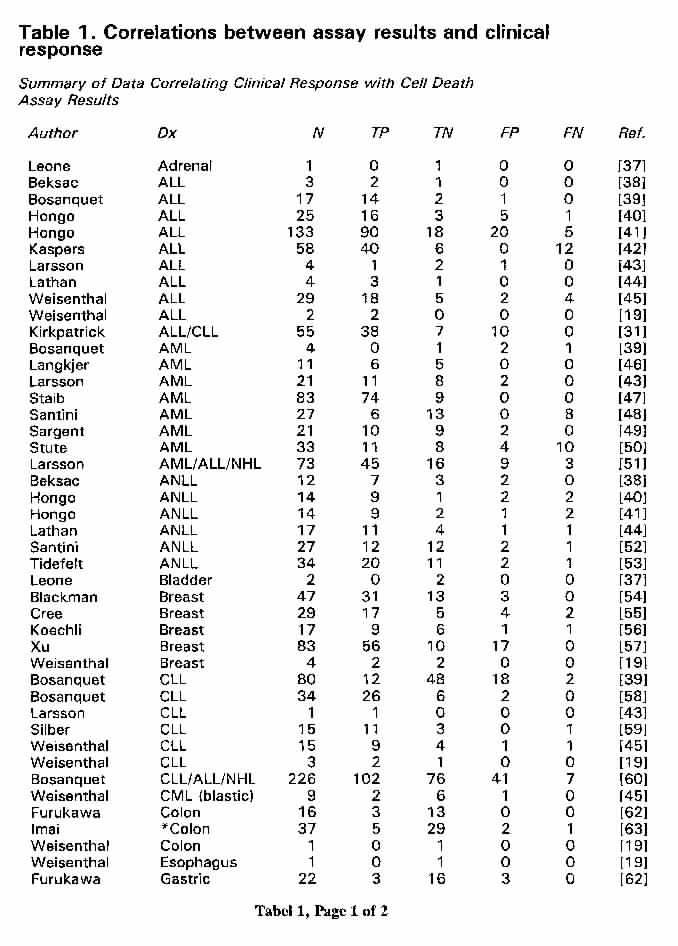
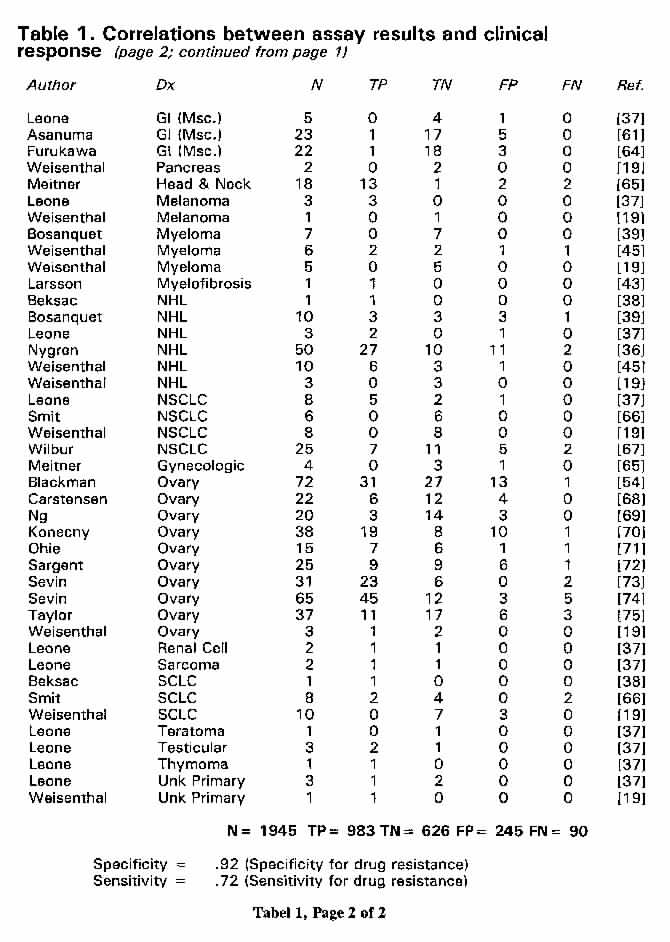
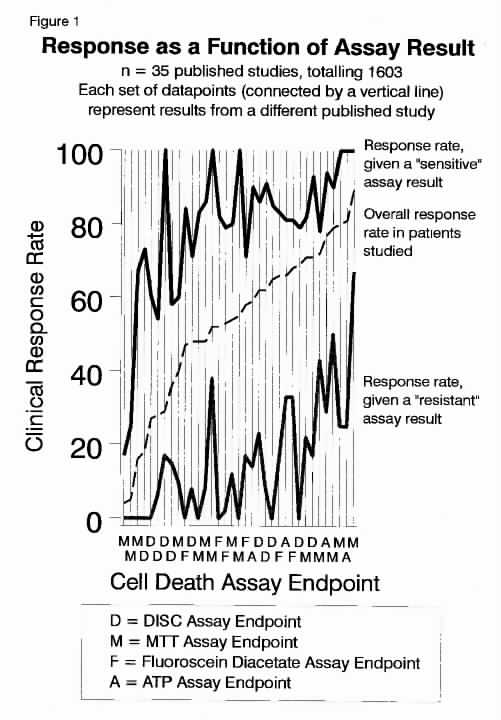
The tables and figures described below show that the above hypothesis has been confirmed to be true in every single study of these assays ever carried out. Table 1 (page 1) and Table 1 (page 2) show the raw published data from which the results were taken, with literature references. Figure 1 shows the results of each individual study, arrayed in order of increasing response rates in the total patient population studied. In every single case, without exception, assay "sensitive" patients were more likely to respond than the total patient population as a whole and assay "resistant" patients were much less likely to respond than the patient population as a whole. In every case, patients treated with assay "resistant" drugs were considerably less likely to respond than patients treated with assay "sensitive" drugs. This should not be a surprising finding. Intuitively, tumors relatively resistant to drugs in vitro would seem, on the whole, to be less likely to respond to the same drugs in vivo. This is precisely what the published data show.
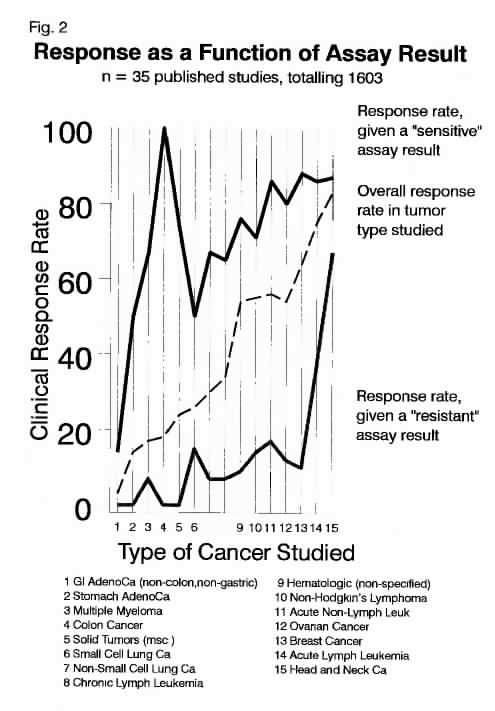
Figure 2 shows the correlations between assay results and treatment, broken down as to histopathologic diagnosis. These are also arrayed in order of increasing overall response rates of the patient populations under study. In each case, assay "sensitive" patients were more likely to respond than the overall patient population and assay "resistant" patients were less likely to respond. In every case, patients treated with assay "sensitive" drugs were more likely to respond than patients treated with assay "resistant drugs." The only "near exception" to this point was in the case of head and neck cancer, in which results were available only from a single study, in only a handful of patients. It may further be concluded from Figure 2 that cell death assays are broadly applicable to a broad range of neoplasms. This does not prove, for example, that the assays are clinically valid for a given rare tumor, such as esthesioneuroblastoma, but there is no reason to expect that the cell death assays should not be valid in any given type of neoplasm.
Return to HTAJ Home Page
Return to Title/Abstract/Chapter Table of Contents
Return to Chapter 2: Cell Death Assays
Proceed to Chapter 4: Assay results in the
context of Bayes' Theorem
{kind=link}
{kind=link}
{kind=link}
{kind=link}