As discussed in the August 7, 2005, editorial on this website ( click here), the clinical trial of Cree, Kurbacher and associates (ASCO Meetings, May, 2005) achieved exceptional chemotherapy response rates in platinum-resistant ovarian cancer, but with no clear improvements in overall patient survival. This study, in the context of the existing clinical trials literature, points to the need for changes in our approach to the chemotherapy of the most common forms of adult cancers.
These investigators had previously used a cell death (ATP endpoint) assay to identify two novel drug combinations: (1) paclitaxel/mitoxantrone and (2) gemcitabine/treosulfan with remarkable activity in platinum-resistant ovarian cancer. Independently, Nagourney, using another cell death (DISC) assay described notable activity for the gemcitabine/cisplatin combination in relapsed ovarian cancer.
Cree and associates recently presented results of a clinical trial in platinum-resistant ovarian cancer in which 105 (out of 159) patients received one of these three regimens as 2nd line therapy and in which many patients subsequently received one of these regimens as third line therapy. They reported a 38% overall response rate to 2nd line therapy and a 40% response rate to third line therapy, both of which are about twice as good as previously reported the literature in large phase II trials. Despite this doubling of response rates, there was no hint of improved overall patient survival (athough the Cree, et al patients comprised an unusually poor prognosis cohort, as discussed elsewhere on this website).
I really do think that the experience in metastatic breast cancer (as discussed in more detail on this website) is very informative. Back in the early 70s, the median survival for metastatic breast cancer was just under two years. Today it is precisely the same...just under two years. Despite scores of prospective randomized trials involving tens of thousands of patients. Response rates have gone up. Some patients unquestionably have their lives prolonged by years. Yet the overall survival rates have not improved.
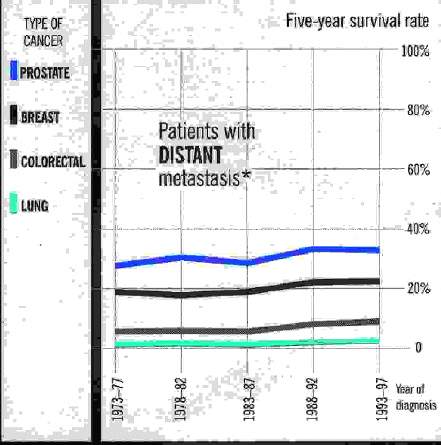
The answer must be that it's all a zero sum game. You give more aggressive chemotherapy (i.e. combinations, high dose therapy, whatever) in diseases like metastatic breast cancer and ovarian cancer and you increase response rates, but you don't improve overall survival. The true situation is NOT that either chemotherapy works or it doesn't. The true situation is that ineffective, aggressive chemotherapy can diminish not just quality of life but also quantity of life -- through organ toxicity, immunosuppression, and/or by inducing mutations in genetically unstable tumor cells to more aggressive phenotypes. The result is no improvement in the treatment of the most common forms of metastatic cancer over the past 30 years (e.g. click here for summary survival graph).
So you want to reserve the aggressive therapy for those patients who will derive more benefit than harm, while identifying the most promising treatment regimens for everyone. In patients with tumors very resistant to cytotoxic chemotherapy in general, the most promising treatments may include angiogenesis inhibitors, growth factor inhibitors, and/or more holistic ("integrative medicine") therapy approaches.
I think it is very important in these clinical trials to try and dissect what is really happening to develop better strategies.
For example, the paradigm for treating recurrent ovarian cancer was, until recently, single agent therapy. It didn't work, because it was all empiric therapy. It could be that the better approach is not to give more aggressive and toxic and mutagenic and immunosuppressive combinations, but to give targeted single agents, or to give least toxic/mutagenic "active" combinations. I think that the Cree study (discussed elsewhere on this website) points in that direction. Higher response rates don't necessarily lead to improved clinical outcomes.
I'm a fan of the gemcitabine/platinum and gemcitabine/alkylator combinations. We've seen anecdotal responses in individual patients which exceed anything I've ever seen or heard about; e.g. our ovarian cancer patient who grew through primary chemotherapy with platinum/Taxol, grew through high dose chemotherapy with tandem stem cell transplants at UCLA, only to achieve a 4 + year duration complete remission (starting with more than a kilogram of pelvic/abdominal/pleural tumor) with gemcitabine/platinum. And our pancreatic cancer patient (0.5 MB PDF) (who presented with advanced disease, with widespread metastases, but who enjoyed a durable complete remission and >7 year survival). But giving this combination to everyone is not all that helpful (subsequent clinical trials in which this regimen was given on an empiric basis to ovarian and pancreatic cancer patients were largely "negative"), because the immunosuppression, mutagenicity, whatever of the combination cancels out, in many patients, the gains in a few, fortunate patients.
In my opinion, the era of empiric, aggressive multi-agent cytotoxic chemotherapy for refractory adult solid tumors should come to an end (or at least be put on vacation until more effective drugs become available). We should, instead, (1) put much more emphasis on matching treatment to patient, though the use individualized testing, (2) have more respect for minimal partial response and/or stable disease, when it can be achieved through the use of least toxic/mutagenic drug regimens, and (3) reserve the use of higher dose therapy and/or agressive combination chemotherapy to those fortunate patients with tumor biologies most amenable to attack and total or near-total destruction by these aggressive treatments.
Larry Weisenthal
August 11, 2005
{kind=link}