Chapter 5: Specific Diseases/Hematologic Neoplasms
The preceding was an overview of the forest of the literature supporting the hypothesis that above-average drug effects in cell death assays correlate with above-average clinical efficacy in the patient, and below-average drug effects in the assays correlate with below-average clinical efficacy in the patient. These (remarkably consistent) data supported the correlation between in vitro and clinical drug effects for a wide range of neoplasms.
We will now consider several individual "trees," or disease types, which have received the greatest amount of study. The diseases considered are (1) lymphatic neoplasms (CLL, ALL, and non-Hodgkin's lymphoma), (2) acute non-lymphocytic leukemia, (3) stomach and colorectal cancer, (4) ovarian cancer, and (5) breast cancer.
(Studies in hematologic neoplasms will be described below, and studies in GI neoplasms, ovarian cancer, and breast cancer will be described in the following Chapter 6)
Lymphatic Neoplasms and ANLL
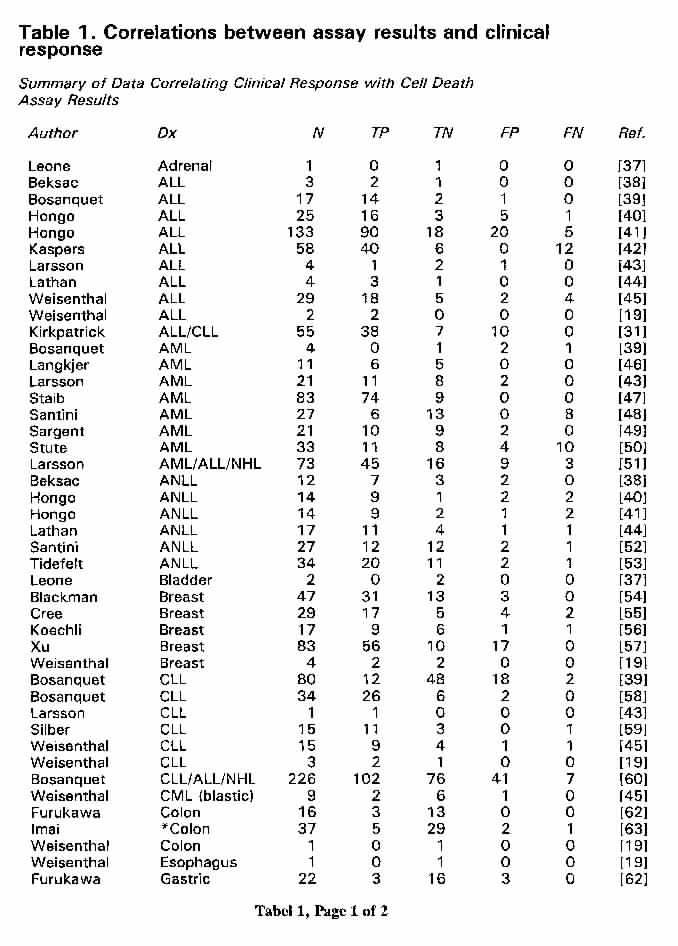
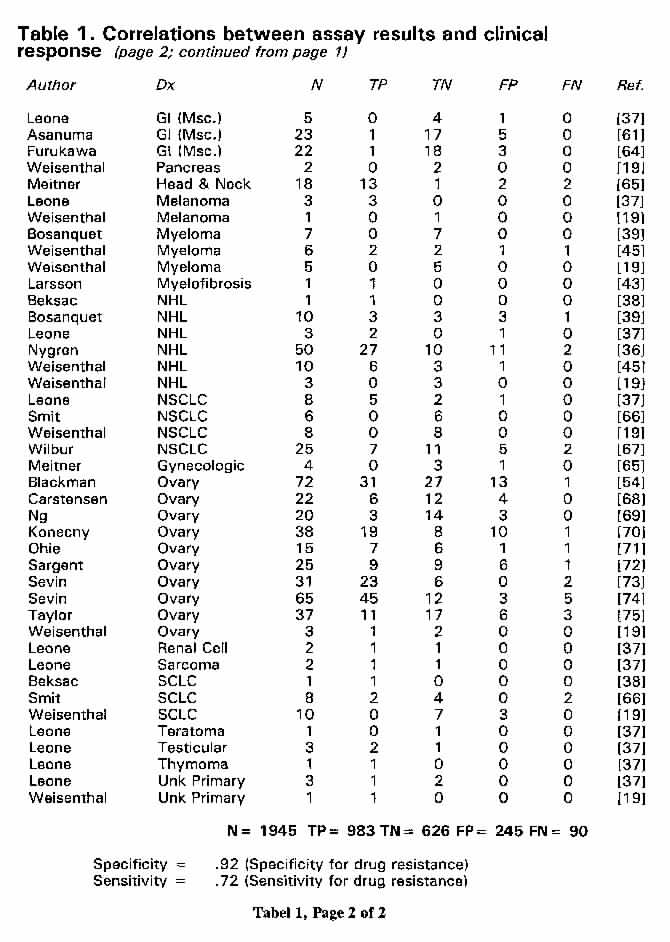
Considering first only correlations between assay results and clinical response (defined as a complete response in the case of acute leukemia and as a partial or complete response for CLL and NHL), Table 1 (page 1) and Table 1 (page 2) show the following correlations:
Acute Lymphoblastic Leukemia: n = 275 published correlations between assay results and response. Overall response rate for patients studied = 76%. Response rates for patients treated with drugs with good activity in the assays = 87%. Response rates for patients treated with drugs with poor activity in the assays = 37%.
CLL: n = 157. Overall response rate = 43%. Response rate with good assay activity drugs = 74%. Response rate with poor assay activity drugs = 6%.
NHL: n = 77. Overall response rate = 55%. Response rate with good assay activity drugs = 71%. Response rate with poor assay activity drugs = 14%.
ANLL: n = 318. Overall response rate = 67%. Response rate with good assay activity drugs = 90%. Response rate with poor assay activity drugs = 23%.
There is a long, extensive, and consistent body of evidence supporting the clinical relevance of cell death assays in human hematologic neoplasms. It is very important to consider this evidence as a whole. One must remember that we are evaluating a laboratory technology and not a therapy. The issue to be considered is the claim that the cell death measured in the assays correlates with tumor cell death measured in the patient. If one considers the CLL and ALL data as a whole, and then also considers the more limited but also consistent data in non-Hodgkin's lymphoma, a very powerful case is made to support the clinical relevance of this testing in human lymphatic neoplasms. If one then goes on to consider the ANLL data in the context of the lymphatic neoplasm data, a powerful case is made to support the clinical relevance of this testing in hematologic neoplasms in general.
The body of literature supporting cell death assays in lymphatic neoplasms dates to studies in CLL published by Schrek in the 1960s [77-80]. Schrek measured the in vitro cell death effects of drugs, heat, and radiation on CLL cells by means of phase contrast microscopy (undoubtedly measuring what we would today recognize as apoptosis and undoubtedly being precisely congruent with the DISC assay). Radiation effects were correlated with clinical outcome [77,80]. Schrek was, non-incidentally, the investigator who first described the identification of viable cells by means of dye exclusion [81].
In the late 1970s, Durkin compared in vitro drug effects in NHL and CLL by means of trypan blue dye exclusion with clinical drug effects and reported good correlations in a small study [82]. Independently, the DISC assay was developed as an improved variation of the trypan blue test, in which suspension cultures of cells were first exposed to trypan blue, spun down onto Cytospin slides, and then counterstained with either Hematoxylin/Eosin or Wright/Giemsa (to identify the non-trypan blue-stained cells with respect to whether these surviving cells were tumor cells or normal cells). With further improvement (substitution of fast green stain for trypan blue and the addition of acetaldehyde-fixed duck erythrocytes as an internal standard to aid in scoring the Cytospin slides), clinical correlations in CLL and other neoplasms were first reported in abstract form and at meetings in the US and Europe in 1981 [83,84].
The first full journal publication of clinical correlations with the DISC assay occurred in 1983 and 1984, which included studies of the activity of glucocorticoids and standard cytotoxic agents correlated with prior therapy and with clinical outcome in ALL and CLL [15,19,85]. This was followed, in 1986, with a study showing the clinical relevance of the DISC assay in CLL, ALL, and NHL using several clinical endpoints: (1) correlations with known disease-specific activity profiles, (2) individual patient correlations with clinical response, (3) greater resistance of specimens from previously-treated patients versus previously-untreated patients, and (4) a shift to significantly greater drug resistance in metachronous assays in the presence of intervening chemotherapy, but no shift in the absence of intervening chemotherapy [45]. It should be noted that these findings were subsequently independently confirmed by other investigators in more comprehensive studies [26,31,36,39,40,43,51,59,86-91]. Additionally, studies in pediatric ALL reported that resistance to dexamethasone in the DISC assay predicted for poor survival [92,93]. These findings were also independently confirmed (see below).
By the late 80s, a number of other investigators had begun to look at the DISC assay and related cell death assays. These began with a head to head comparison of the DISC assay with the MTT assay in established cell lines by the NCI lung cancer group [20,27]. These studies established the comparability of these endpoints in homogeneous cell populations.
A group at the Free University of Amsterdam carried out a head to head comparison of the DISC endpoint with the MTT endpoint in acute lymphoblastic leukemia [29,30]. This group showed that the endpoints were comparable in specimens in which the percentage of leukemia cells (relative to normal cells in the specimen) was greater than 80 [29,30,94]. This group found the MTT endpoint to be much less labor intensive. They used the same general conditions originally described for the DISC assay (including a 96 hour continuous drug exposure, followed by comparisons between drug exposed and control cultures with the cell death endpoint). These Dutch authors went on to publish an extensive, elegant, and ongoing series of rigorous studies which have established that the assay results correlate with and predict for both response and survival in ALL, and that the assay results are, in fact, the only factor which independently predicts for survival in pediatric ALL [87,88,90,95-103]. They have also extended this work to ANLL [89,104,105]. Taken in the context of the entire literature, these studies in pediatric ALL provide complementary support for the validity of complementary studies in CLL (described below).
Other investigators also showed strong correlations between cell death assay results and clinical outcome (response and/or survival) in pediatric ALL [40,41,91-93,106], adult ALL and ANLL [25,31,44,46,47,49,52,53,99,107-113], CLL [58,59,114-116], and adult NHL [19,36,45,51]. These studies included further confirmation of the comparability between DISC and MTT endpoints in assays on clinical specimens and also introduced the fluorescein diacetate cell death endpoint, which, like the DISC endpoint, measures cell membrane integrity and which correlates very well with the DISC endpoint in homogeneous cell populations [26,36].
In 1991, Bosanquet published in Lancet a relatively large number of correlations between clinical response and DISC assay results, chiefly in CLL [39]. He showed, furthermore, highly significant correlations between assay results and patient survival. This paper also confirmed the relevance of the "EDR" (extreme drug resistance) endpoint, which is defined as an assay result more than one standard deviation more resistant than the median of comparison assays. Bosanquet later described a paradoxical shift toward increased methylprednisolone sensitivity in previously-treated CLL and used the DISC assay to identify high dose methylprednisolone as an effective treatment for otherwise refractory CLL [117,118].
These studies with the DISC and MTT assays are supported by studies with the fluorescein diacetate (FDA) endpoint. Fluorescein diacetate is a lipid soluble material which readily penetrates cell membranes. Viable cells contains a membrane esterase which cleaves the dye to non-lipid soluble fluorescein, which is concentrated in cells containing a functionally-intact membrane. Thus, the assay is conceptually similar to the DISC assay, which measures the ability of cells with functionally-intact membranes to exclude non-lipid soluble dyes. Delayed loss of this membrane integrity is a marker of apoptotic cell death [119].
Investigators at Uppsala University in Sweden began work in the 1980s by comparing the DISC and FDA assays and establishing their comparability [26,36,51]. They proceeded to publish a series of studies showing (1) strong correlations with assay results and treatment outcomes in NHL and ANLL [25,26,43,107,108,120], (2) confirming the specificity of the EDR endpoint in predicting for clinical non-response [108], and (3) confirming and extending earlier reports of the capability of the cell death endpoint to identify the general disease-specific activity patterns of a diverse spectrum of drugs [86,121].
Within the past several years, additional studies have provided strong support for the clinical relevance of the information provided by cell death assays in hematologic neoplasms.
Bosanquet and colleagues reported a study in 243 CLL patients [116]. "Standard" first-line chemotherapy in the USA is fludarabine, but there are acceptable alternatives, such as single agent chlorambucil, cyclophosphamide, cladribine, and combinations such as "CVP" (cyclophosphamide/vincristine/ prednisone). In Bosanquet's study, fludarabine-sensitive patients treated with fludarabine had a 69% response rate (80% for untreated patients; 64% for previously-treated patients), while fludarabine-resistant patients had a 7% response rate (25% for previously-untreated; 0% for previously-treated). 66 patients received fludarabine within a year of the performance of the DISC assay. 15 of these were test-resistant. Not a single one of these 15 patients resistant to fludarabine but treated with fludarabine survived 17 months, and their median survival was 7.9 months. In contrast, the fludarabine-sensitive patients treated with fludarabine had an 80% chance of surviving beyond 17 months, a 41.7 month median survival, and a 25% chance of surviving beyond 6 years. Patients with DISC assay resistance to fludarabine, but treated with other regimens than fludarabine had a median survival of 16.3 months and 10% survived beyond 4 years. The relative risk of death for patients with DISC assay fludarabine resistance treated with fludarabine versus treated with a non-fludarabine regimen was 2.9. On multivariate analysis, fludarabine test resistance was a more important determinate of survival in patients treated with fludarabine than was any other clinical characteristic, including sex, Binet stage, prior chemotherapy, and patient age. In a separate analysis, DISC assay-directed therapy of CLL was calculated to be cost effective [122].
Other investigators, as noted, have reported that assay results are important predictors of patient survival in pediatric acute lymphoblastic and non-lymphoblastic leukemia [103,123-126].
Similar studies have been reported for adult acute non-lymphocytic leukemia [47,53,111,127]. Three different groups have published strong correlations between CCDRT results and survival in ANLL. Correlations between DISC assay results and patient survival in ANLL were first published by a Swedish group in 1989 [53]. These results were recently confirmed and extended by a group at the University of Cologne [47,111], in follow-up to their earlier report of strong correlations between DISC assay results and clinical remission of adult acute non-lymphocytic leukemia a decade earlier [44]. In their recent follow-up studies, the DISC assay results "precisely" predicted clinical outcome, and identified a group of patients with a 100% early death rate, when treated with conventional induction therapy [47]. These studies are very analogous to Bosanquet's work identifying a group of CLL patients in whom conventional treatment is uniformly fatal.
The German group followed up with a presentation at the American Society of Hematology (ASH) meetings in December, 1999, in which multivariate analysis showed DISC assay results to be the strongest factor predicting for clinical outcome in adult ANLL [111]. Most recently, a Danish group reported studies correlating MTT assay results with both overall and relapse-free survival in 85 adult ANLL patients [127]. Assay results remained significantly correlated with survival on multivariate analysis. This work on ANLL is precisely analogous and complementary to the studies by the Dutch (Amsterdam) group in pediatric ALL, discussed above.
The only "negative" study ever published concerning total cell kill (cell death) assays in hematologic neoplasms was an otherwise "positive" study in adult acute non-lymphocytic leukemia, in which strong correlations between anthracycline activity and survival were shown, but poor correlations between cytarabine activity and survival were seen [113], in contradistinction to several other studies in which assay results with cytarabine were found to be strongly correlated with patient survival [47,53,104,111]. The "negative" study was the only one to use the ATP endpoint, which is disadvantageous in hematologic neoplasms, as normal cells, red blood cells, and platelets all produce an appreciable "contaminating" ATP signal, in contradistinction to the other cell death endpoints, which are less affected by such artifacts. The authors of the "negative" cytarabine study acknowledged that they did not determine the percentage of leukemic blast cells at the conclusion of the cell culture and noted the advantages of the DISC assay in being able to discriminate neoplastic from normal cells.
Thus we have, in hematologic neoplasms, a 35 year history of highly positive studies, published by investigators in the USA, the United Kingdom, the Netherlands, Germany, Sweden, Canada, Italy, and Japan all showing consistent, strong correlations between the results of cell death assays and clinical outcomes. In summary, there is a strong scientific rationale for these tests and that the clinical relevance of the information provided by the tests has been documented in a collectively large and diverse literature in hematologic neoplasms.
Return to HTAJ Home Page
Return to Title/Abstract/Chapter Table of Contents
Return to Chapter 4: Assay results in the
context of Bayes' Theorem
Proceed to Chapter 6: Specific Diseases/Solid
Tumors
{kind=link}
{kind=link}