Chapter 4: Assay Results in the Context of Bayes' Theorem
The absolute predictive accuracy of the tests varies according to the overall response rate in the patient population being studied, in accordance with Bayesian principles [76].
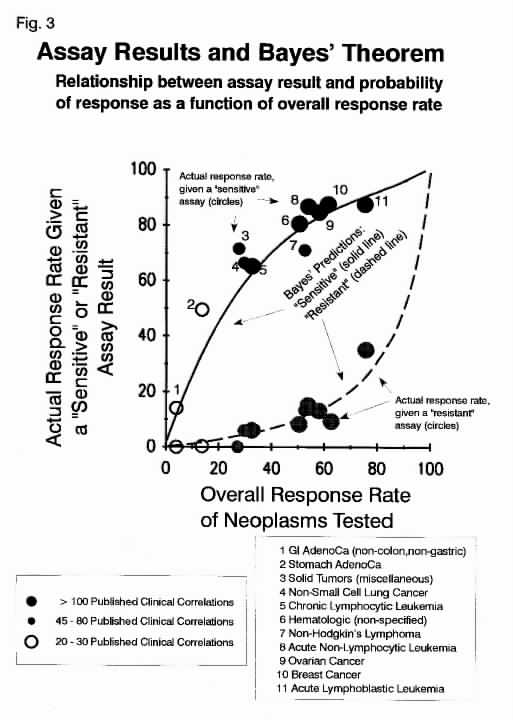
Figure 3 is of greatest importance, and is well worth considering. If one understands this figure, one goes a long way to understanding how the results of these assays should be used in patient management. The solid and dashed lines in this figure show the theoretical expectations for the cell death assays, based on Bayes' Theorem, applied to assays with an overall specificity for drug resistance of 0.92 and an overall sensitivity of 0.72, which represent the overall findings from the studies included in the meta-analysis. The circles show the actual response rates of patients with different types of neoplasms, given that either "sensitive" or "resistant" results were obtained. It may be seen that, in every case, the actual performance of the assays in each type of tumor precisely matched predictions made from Bayes' Theorem, projected from the overall assay sensitivity and specificity.
The findings in Figure 3 show conclusively that the cell death assays are broadly applicable to a wide range of human neoplasms, ranging from low response rate tumors, such as pancreatic cancer and cholangiocarcinoma (group 1, the non-colon, non-stomach GI adenocarcinomas) to acute lymphoblastic leukemia (group 11), and including breast cancer and ovarian cancer.
Of equal importance, this figure shows how the assay may be best applied to patient management decisions. It is obvious that, in high response rate neoplasms, there will be many "false negative" predictions. No one should ever use these assays to deny chemotherapy to such patients, if chemotherapy is otherwise indicated, any more than one should deny antibiotics in an infection with an in vitro drug resistant bacterium. In cases where there is one particular drug regimen which has been shown to produce a very high cure rate and this regimen is widely accepted as being superior to all other regimens (e.g. testicular cancer, where dose-intense cisplatin/etoposide/bleomycin has been shown to produce the highest cure rate), it would be most unwise to forgo this regimen solely on the basis of today's available cell culture assays.
On the other hand, the assays could be appropriately used to identify patients with above and below-average clinical prognoses if treated with given drugs. In cases where more than one acceptable regimen exists, the physician could select the regimen containing the most favorable drugs and avoid the regimen containing the most unfavorable drugs. This would apply to clinical decisions at all points along the curve. Thus, the absolute probability of response with assay "sensitive" and "resistant" drugs varies according to the overall prior response probability in the patient population studies, but, at all points, assay "resistant" patients have a below average probability of response and assay "sensitive" patients have an above average probability of response and treatment with assay "sensitive" drug(s) is more likely to be associated with a favorable outcome than treatment with assay "resistant" drugs.
Return to HTAJ Home Page
Return to Title/Abstract/Chapter Table of Contents
Return to Chapter 3: Correlations between assay
results and chemotherapy response
Proceed to Chapter 5: Correlations in Specific
Diseases/Hematologic Neoplasms
{kind=link}